On August 5th, 2003, I underwent Weight Loss Surgery (WLS). My research started June of 2002 on the effects, benefits, and risk of this type of surgery. I had been over weight most of my life, only able to lose excess weight with the help of amphetemines.
July of 2002, I visited my primary care physician, Dr. Mary Mahern of Bloomington, IN. Dr. Mahern totally supported me and got the ball rolling. I had a complete physical...from top to bottom! LOL! At this time I had a BMI of 40, and weighed 216 lbs. I am only 5'2". My co-morbidities included Fibromyalgia, Acid-Reflux, Joint Pain, Shortness of Breath, and Depression. I was taking a total of around 10 pills a day for these problems.
August 27th of 2002 I had my first visit with my surgeon to be, Dr. Margaret Inman of Indianapolis, IN. Dr. Inman was very informative and thorough. She tells it like it is...giving the pros and cons. It was very cut and dry...either you were going forward with the surgery or you weren't...I knew I was going forward before I left Dr. Inman's office.
I came home and wrote a letter to my insurance company, in detail, explaining why I needed to have this surgery and what my life had been like being ill for several years due to obesity. Dr. Inman's office sent in all paper work informing the insurance why this surgery was a medical nessecity for me. Dr. Mahern sent in a letter of reference as well. I was approved for surgery in less than 4 weeks!
I had to request my surgery date for almost a year later due to being accepted into the nursing program at Ivy Tech State College. Time went very quickly!
Surgery went smoothly...but I awoke wondering what the hell I had done!! I couldn't get out of bed without help...I couldn't walk standing straight up...depression set in quickly. I was in the hospital for almost 4 days. And daily I would think about what a mess I was...how could I alter my body and put myself through total HELL?!?!?! The "head-hunger" was horrible for weeks. I would spend a lot of time lying in my bedroom, crying non-stop. I didn't want to be around anyone or even talk to anyone. I was TOTALLY miserable! I had to have 3 endoscopes due to my openings closing. I finally started to heal and everything stayed open.
It's been 4 1/2 months since my journey began. It has not been pleasant, nor has it been easy...and it never will! Eating is not a problem...I pretty much eat what I want in very small amounts. I try to stay away from sugar as much as possible. Over eating or eating something that doesn't agree with your...pouch...is NOT a pleasant experience! I still have probs with nausea, and I don't eat as much as I should. I do take my vitamins faithfully plus a V-B12 injection monthly. I am down to one pill daily...well...nightly. I do take Ambien at bedtime, I hope to be able to stop that medication sometime in the near furture. My BMI is down to 29.6 at this time, and my weight at 162 lbs. I've also went down 3 clothes sizes. But unfortunately...I'm still only 5'2"!! LOL!!
Christmas Eve, Dec. 24th, 2003
4 1/2 Months Post-op
Weight 162 lbs
It is now January 2005, it has been 1 year and 5 months since my surgery. I have lost 100 lbs and weigh in around 120 - 123 lbs., my BMI is 22.3...I'm in the normal range for once in my life!! I usually wear a size 5 in pants and a small or medium in tops. Remember, I started out at a size 20 and XXL, so this is an enourmous change for me. I still have to look twice whenever I glance in a mirror.
Me, my Beautiful Mother & my sis Kammi
November 11th, 2003
15 Months Post-op
Weight 121 lbs
The major probs I have had is with my kidneys. I have had so many stones I've lost count. My urologists and I have become friends. LOL!! I've had 4 or 5 lithotripsys and 1 dialation in the past year. Nausea isn't too bad anymore, but I still don't eat as much as I should. Some days I want to eat, some days I can't stand the thought of food!!
WLS isn't something to take lightly(no pun intended!). I still can't say I am 100% glad I did it. This is a TOTALLY body and life altering surgery. It is something that needs researched intensely. It is a decision only you can make for yourself...by yourself!
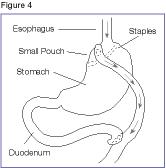
Roux-en-Y gastric bypass (RGB)
This operation, illustrated in figure 4, is the most common and successful malabsorptive surgery. First, a small stomach pouch is created to restrict food intake. Next, a Y-shaped section of the small intestine is attached to the pouch to allow food to bypass the lower stomach, the duodenum (the first segment of the small intestine), and the first portion of the jejunum (the second segment of the small intestine). This bypass reduces the amount of calories and nutrients the body absorbs.
Malabsorptive operations produce more weight loss than restrictive operations, and are more effective in reversing the health problems associated with severe obesity. Patients who have malabsorptive operations generally lose two-thirds of their excess weight within 2 years.
In addition to the risks of restrictive surgeries, malabsorptive operations also carry greater risk for nutritional deficiencies. This is because the procedure causes food to bypass the duodenum and jejunum, where most iron and calcium are absorbed. Menstruating women may develop anemia because not enough vitamin B12 and iron are absorbed. Decreased absorption of calcium may also bring on osteoporosis and metabolic bone disease. Patients are required to take nutritional supplements that usually prevent these deficiencies. Patients who have the biliopancreatic diversion surgery must also take fat-soluble (dissolved by fat) vitamins A, D, E, and K supplements.
RGB and BPD operations may also cause “dumping syndrome.” This means that stomach contents move too rapidly through the small intestine. Symptoms include nausea, weakness, sweating, faintness, and sometimes diarrhea after eating. Because the duodenal switch operation keeps the pyloric valve intact, it may reduce the likelihood of dumping syndrome.
The more extensive the bypass, the greater the risk for complications and nutritional deficiencies. Patients with extensive bypasses of the normal digestive process require close monitoring and life-long use of special foods, supplements, and medications.
Surgery to produce weight loss is a serious undertaking. Anyone thinking about surgery should understand what the operation involves. Patients and physicians should carefully consider the following benefits and risks:
Benefits
* Right after surgery, most patients lose weight quickly and continue to lose for 18 to 24 months after the procedure. Although most patients regain 5 to 10 percent of the weight they lost, many maintain a long-term weight loss of about 100 pounds.
* Surgery improves most obesity-related conditions. For example, in one study blood sugar levels of 83 percent of obese patients with diabetes returned to normal after surgery. Nearly all patients whose blood sugar levels did not return to normal were older or had lived with diabetes for a long time.
Risks
* Ten to 20 percent of patients who have weight-loss surgery require follow-up operations to correct complications. Abdominal hernia was the most common complication requiring follow-up surgery, but laparoscopic techniques seem to have solved this problem. In laparoscopy, the surgeon makes one or more small incisions through which slender surgical instruments are passed. This technique eliminates the need for a large incision and creates less tissue damage. Patients who are superobese (>350 pounds) or have had previous abdominal surgery may not be good candidates for laparoscopy, however. Less common complications include breakdown of the staple line and stretched stomach outlets.
* Some obese patients who have weight-loss surgery develop gallstones. Gallstones are clumps of cholesterol and other matter that form in the gallbladder. During rapid or substantial weight loss, a person’s risk of developing gallstones increases. Taking supplemental bile salts for the first 6 months after surgery can prevent gallstones.
* Nearly 30 percent of patients who have weight-loss surgery develop nutritional deficiencies such as anemia, osteoporosis, and metabolic bone disease. These deficiencies usually can be avoided if vitamin and mineral intakes are high enough.
* Women of childbearing age should avoid pregnancy until their weight becomes stable because rapid weight loss and nutritional deficiencies can harm a developing fetus.
Gastrointestinal surgery may be the next step for people who remain severely obese after trying nonsurgical approaches, or for people who have an obesity-related disease. Candidates for surgery have:
* a BMI of 40 or more
* a life-threatening obesity-related health problem such as diabetes, severe sleep apnea, or heart disease and a BMI of 35 or more
* obesity-related physical problems that interfere with employment, walking, or family function.
If you fit the profile for surgery, answers to the following questions may help you decide whether weight-loss surgery is appropriate for you.
Are you:
* unlikely to lose weight successfully with nonsurgical measures?
* well informed about the surgical procedure and the effects of treatment?
* determined to lose weight and improve your health?
* aware of how your life may change after the operation (adjustment to the side effects of the surgery, including the need to chew well and inability to eat large meals)?
* aware of the potential for serious complications, dietary restrictions, and occasional failures?
* committed to lifelong medical follow-up?
: There are no guarantees for any method, including surgery, to produce and maintain weight loss. Success is possible only with maximum cooperation and commitment to behavioral change and medical follow-up—and this cooperation and commitment must be carried out for the rest of your life.