 Original Article
Original Article
The world over thymectomy is standard therapy for myasthenia gravis. When there is no thymoma, thymectomy is followed by improvement in 66 to 86% of the patients(1). The choice of operative approach, i.e. transcervical, transsternal or the so called "maximal" thymectomy still remains controversial.
In the period from may 1982 to may 1997 we performed 80 transcervical thymectomies using a sternal suspension technique. To improve thymectomy by this approach we perform an artificial pneumomediastinum as a means to air dissect the soft tissues around the thymus and thus facilitate the surgical dissection of the gland.
TECHNIQUE
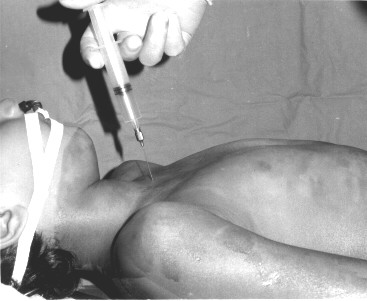
Following anesthesia, with the patient supine, a puncture is made in the suprasternal notch using a curved 8 gauge BD lumbar needle which tip is introduced in the soft tissues of the anterior mediastinum behind the manubrium sterni (Figure 1).
With a syringe manual suction is applied to the needle to rule out the presence of blood. The table is adjusted to a 45 degree Trendelemburger position. Air is then gently and slowly injected into the mediastinum usinf a 10 cc syringe. The amount of air injected varies from 300 to 600 cc (Figure 2).

A small horizontal cervical incision is made and the straight muscles of the neck are retracted. The presence of air is noticed scaping from the soft tissues of the anterior mediastinum allowing a better identification of the borders of the upper poles of the thymus lobes in front of the trachea. The air infiltrating the connective tissues that surrounds the thymus greatly improves the surgical dissection of the thymic vein and of the lateral and posterior aspects of the gland in its relationship with both mediastinal pleurae and the innominate vein.
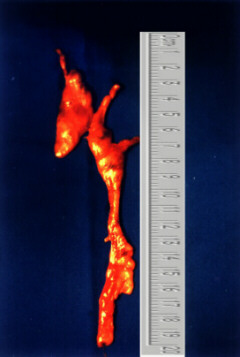
The manubrium sterni is suspended, and following ligature of the thymnic vein the dissection of the rest of the gland is best performed under direct vision using long straight scisors and Boseman's clamps.(Figure 3)
COMMENTS
Pneumomediastinography (artificial pneumomediastinum) was introduced in the radiological investigation of the thymus by Apert in 1939 for the diagnosis of thymic hypertrofy(2). In 1964 Bariety and Coury reported their experience with 675 cases of pneumomediastinography, and pointed out its value as a diagnostic procedure, particularly for the diagnosis of thymic tumours(3). In 1967 Coury and Chedru further emphasized the value of the method in the diagnosis of small thymic tumours that were not detected by chest X-ray or conventional tomography (4). According to these authors the method is well tolerated and air can be injected with only small substernal disconfort felt by the patients.With the advent of CT scans, pneumomediastinography is in disuse.
We use the artificial pneumomediatinum as a technical tool to make easy thymectomy by the cervical approach(5). When there is no intense perithymic inflammation and adhesions, performing an artificial pneumomediastinum greatly facilitates the dissection of the gland, specially around the innominate vein and improves dissection of the thymus under direct vision.
No complications occurred related to the use of pneumomediastinum in this group of patients. It is our opinion that pmeumomediastinum technically improves thymectomy by the cervical approach.
REFERENCES
(1)Prowland L. Controversies about the treatment of myasthenia gravis. J. Neurol. Neurosurg. Psychiatry., 1980;43:644-659.
(2)Apert E. Le pneumomédiastin anterieur. Méthode diagnostique dans les formes atypiques d'hypertrophie du thymus. Nourisson., 1939;27:91.
(3)Bariety M, Coury C. Importance de la médiastinographie gazeuze dans le diagnostic radiologique des tumeurs du thymus. Canad. Med. Ass. J., 1964;90:517.
(4)Coury C, Chedru F. Physiologie et pathologie du thymus. Le Poumon et le Coeur., 1967;38:881.
(5)Urschel,Jr. HC and Cooper JD. Atlas de Cirurgia Torácica. Livraria e Editora Revinter, Rio de Janeiro, 1997, pp.68-73.

