-
Laboratory methods:
| -
Cell culture:
- Nucleic acid
detection in clinical specimens:
|
- Cell culture:
Culture detects
only viable infectious chlamydial elementary bodies and has minimal
potential for contamination. With the advent of DNA amplification techniques,
culture tests are used less frequently and are generally now performed
only in specialized reference laboratories.
Culture is performed
by inoculating specimens onto cell culture monolayers. If
sufficient numbers of viable chlamydial elementary bodies are present,
they infect the cells and grow to form intracytoplasmic inclusions.
Cell monolayers
for culture of C.trachomatis are grown in dram or shell vials on glass
coverslips or in the wells of multiwell cell culture dishes. Traditionally,
Mc Coy and HeLa 229 cells have been use to support the growth of C.trachomatis.
The susceptibility of HeLa 229 cells to infection is increased by pretreatment
with DEAE-dextran. The same effect is seen with uncentrifuged Mc Coy cell
monolayers.
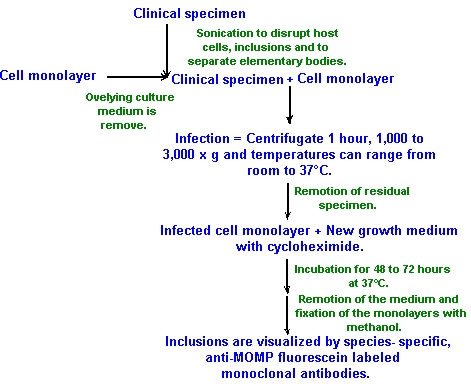
Before the inoculation
is made, clinical specimens should be sonicated to disrupt host cells and
inclusions and to separate elementary bodies. If a sonicator is not available,
specimens should be vortex thoroughly or can be disrupted with glass beads.
To inoculate
the cell cultures, the overlying culture medium should be first be removed
and replace with enough of the specimen in culture transport medium to
cover the monolayer and prevent drying during subsequent centrifugation.
Shell
vials are centrifugated to enhance culture sensitivity for 1hour at
1,000 to 3,000 x g temperatures that can range from room temperature to
37°C. The potential for a cytotoxic effect of the specimen on the monolayer
is minimized by removal of the residual specimen after centrifugation by
aspiration and overlaying the monolayer with fresh cell culture medium.
Once inoculated, host monolayers should be incubated in growth medium containing
cycloheximide
(0.5 to 1.5 mg/ml)
to selectively inhibit host cell protein synthesis. Inoculated monolayers
are then incubated for 48 to 72 hours at 37°C. After incubation,
the medium is removed and the monolayers are fixed with methanol.
The inclusions
are visualized following incubation by staining with fluorescently labeled
antibodies that bind chlamydial lipopolysaccharide (LPS) to recognize
all chlamydial species, or major outer membrane protein (MOMP) for C.trachomatis-specific
recognition. The preferred method for identification of inclusion is to
stain infected monolayers with species-specific, anti-MOMP fluorescein-labeled
monoclonal antibodies.
Some
stains as Gram, iodine or Giemsa have been used to visualize chlamydial
inclusion in cell culture, but these are not commonly used today due to
lack of sensitivity and specificity compared to fluorescent-antibody staining.
The antigen detection
assays (nonculture) commercially available for the detection of C.trachomatis
in clinical specimens utilize either monoclonal or polyclonal antibodies
directed against Chlamydia genus-specific LPS or specific or Chlamydia
specific MOMPs as capture or detector reagents. One of several types of
chemical labels is conjugated to the detector antibody or antibodies in
the assay. Fluorescein isothiocyanate is conjugated to the detector in
the
DFA method, whereas various enzymes may be used in the EIA
or microparticle immunoassays (MEIA) in which 96-well plates, beads,
or microparticles are used to trap the C.trachomatis antigens. Depending
on the substrate used for the enzyme to act on, the signal measured in
the EIAs is a color change or chemiluminescence. All of these nonculture
antigen methods have similar sensitivities and specificities when compared
to the cell culture.
Serological assays
are valuable epidemiology tools and can help in the diagnosis of systemic
infections such as pneumonia, ectopic pregnancy or tubal factor infertility
where antibody titers are often elevated.
There are serological
assays that detect antibodies common to all members of the genus. The most
common are complement fixation (CF), recombinant enzyme-linked immunofluorescence
(rELISA), and whole inclusion immunofluorescence (WIF), which are mainly
based on the detection of LPS.
* Complement fixation:
Detects complement-fixing antibodies that recognize the genus-specific LPS antigen and is not specific for any one chlamydial species. Treatment with antibiotics can delay or dismiss the production of CF antibody and will reduce the sensitivity of the test.
* rELISA:
This test detect reactivity to genus-specific antigen, or LPS, of chlamydial elementary and reticulate bodies.Now, these tests are commercially available.
* Microimmunofluorescence (MIF):
The MIF test
is the most sensitive of the serologic tests for Chlamydia species and
the only serologic test that detects species-specific responses. It is
based on the visualization of elementary bodies or reticulate bodies instead
of intact inclusions. This assay, which can measure responses to subclasses
IgM, IgA, and IgG, is technically demanding, requiring a well-trained and
experienced reader, and thus should be performed only in highly specialized
laboratories.
- Nucleic acid detection in clinical specimens:
* Amplified nucleic acid assay:
The development
of tests based on nucleic acid amplification technology has been the most
important advance in the field of chlamydial diagnosis since in vitro cell
culture techniques replaced the yolk sac for culture and isolation of the
organism from clinical specimens.
Nucleic
acid amplification is exquisitely sensitive, capable of detecting
as little as a single gene copy, and highly specific. It offers
the opportunity to use noninvasive sampling techniques to screen for infections
in asyntomatic individual who would not ordinarily seek clinical care.
- PCR (Polymerase chain reaction): The PCR test employs two synthetic oligonucleotide primers (15-30 base pairs) with sequences that are complementary to flanking regions of a specific DNA segment present in the target organism. PCR can be genus, species, group, or strain specific depending on the primer design. A target DNA template in clinical specimens must be made available to the primers by detergent-or heat-mediated lysis of organisms and denaturation of double-stranded DNA. Once the primers are hybridized to the DNA template (one per DNA strand), they are extended into DNA products of a length determined by the distance between the two primer annealing sites. The primer are extended through the activity of a thermostable DNA polymerase enzyme, most commonly Taq polimerase (come from Thermus aquaticus bacteria). The double-stranded PCR products become templates for a second round of primer annealing upon denaturation. Multiple cycles of denaturation, annealing, and extention of products result in a logarithmic amplification of the DNA target segment. The PCR products, also called amplicons, are detected by electrophoresis and staining with a DNA intercalating fluorescent dye as ethidium bromide.
The PCR reactives are:
 -
PCR test
-
PCR test
- LCR (Ligase chain reaction): The LCR test employs four
synthetic oligonucleotide probes (two per DNA strand) anneal at specific
target sites on the cryptic plasmid. Each pair of probes hybridize close
together on the target DNA template, with 1- to 2- nucleotide gap between.
Once the probes are annealed, the gap is filled by DNA polimerase and close
by the ligase enzyme.. This two-step process of closing the gap between
annealed probes makes the LCR, in theory, more specific than PCR technology.
The ligated probe pairs anneal to each other and, upon denaturation, from
the template for successive reaction cycles, thus producing a logarithmic
amplification of the target sequence. Like PCR, LCR is made in a thermocycler.
The LCR product is detected in an automated instrument that uses an immunocolorimetric
bead capture system. At the end of the LCR assay, amplified products are
inactivated by the automatic addition of a chelated metal complex and a
oxidizing agent.
Currently, there is only a single commercially available DNA probe for detection of C. trachomatis (Gen-Probe). This test employs a chemiluminiscent DNA probe. The probe hybridizes to a species-specific sequence of chlamydial 16s rRNA. Once the DNA-rRNa hybrid is formed, it is adsorbed onto a magnetic bead and the chemiluminiscent response is detected quantitatively with a luminometer. Since actively dividing Chlamydiae containing up to 10e4 copies of 16s rRNA, this test should theoretically be more sensitive than antigen detection systems.