
You are visitor number:
Nd: YAG Laser Hyperthermia in The Treatment of Warts :
New Modification of A New Technique.
![]()
Mohammed H. El-Tonsy, Tag E.E Anbar, Talal A. Abd El-Raheem
Abstract: Hyperthermia has for many years been investigated as a way of destroying diseased tissue. The general principle in the treatment of cutaneous diseases with heat is based on the fact that diseased tissue is more sensitive to the effects of elevated temperature than normal tissue and thus is less able to recover after heat exposure. Nd:YAG laser hyperthermia (Regensburg's Technique) was used in the treatment of verrucae vulgaris. This study was conducted with the aim of evaluating the Regensburg's technique and decreasing the number of treatment sessions and increasing success rate through modification on the power energy and time of temperature maintenance. The study was conducted on 40 patients, in each patient the lesions were subdivided into two equal treatment subgroups. One subgroup was treated by Regensburg's technique and the other by Modified Regensburg's technique Modified Regensburg's technique showed a 60 % total cure rate after one treatment session compared to 15 % in the Regensburg's technique, and 100 % total cure rate in. Modified Regensburg's technique after two sessions compared to 45 % in the Regensburg's technique. While 55% of the Regensburg's technique patients required a third treatment session and 20% required a fourth treatment session. The remaining 5% of Regensburg's technique were not cured even after the fourth session. Based on these results, Modified Regensburg's technique appears to be more superior than Regensburg's technique in treating warts with a higher success rate in a shorter number of treatment sessions. No side effects were noted in both techniques, except for two patients (5%) of the Modified Regensburg's technique who required local anesthesia due to their pain intolerance
Introduction
Verrucae vulgaris are, benign cutaneous tumors caused by the human papillomavirus (HPV). Impairment of the epithelial barrier function by any kind of trauma or by maceration predisposes to inoculation by the virus. They are pleomorphic and can be located almost anywhere on the skin surface, but commonly on the hands Department of Dermatology / STD & Andrology, Faculty, of Medicine, El-Menia University. and feet, genital skin and mucosa(l). No completely successful method of treatment of warts yet exists. The lack of antipapillomavirus agents prevents a specific treatment related to the cause. Varying degrees of remission could be obtained with conservative or surgical methods(7).
ĀĀĀHeat therapy of cutaneous diseases has been used for decades. This controlled localized heating was used in veterinary medicine for the treatment of benign(3) and malignant lesions (4,5). In humans, a variety of superficial and deepseated tumors have been treated by hyperthermia with different degrees of successf67). Hyperthermia has been used for the treatment of cutaneous leishmaniasis (8,9) and mycobacterium chelonae(l0), since these organisms do not thrive at temperatures above 39-40 ░C. The general principle of this treatment is based on the fact that diseased tissue is more sensitive to the effects of elevated temperature than normal tissue(11). During the 1960s ultrasound heating of warts was first reported, but was abandoned because of poor response rates, possibly as a result of inefficient treatment schedules(l2,14). In 1992, Sterm and Levine evaluated the effect of hyperthermia on verrucae vulgaris using radiofrequency current. They reported 86% complete regression rate in four treatment sessions(11) In 1995, Pfau et al. used Nd: YAG laser hyperthermia (Regensburg's Technique(12,13) ) with a 77.4% success rate for recalcitrant verrucae vulgaris. Their parameters were using an energy power of 10W, spot size of 8mm and surface temperature of 40 ░C which was maintained for one minute. The inspire of this study was finding that different results were obtained through accidental variation of the parameters during treatment of our patients with Regensburg's technique.
ĀĀĀThis study was conducted with the aim of evaluating the Regensburg's technique and trying to change the parameters with the aim of decreasing the number of treatment sessions and increasing the success rate.
Patients and Methods
Regensburg's Technique(15,16) (RT) .
ĀĀĀNd: YAC laser hyperthermia was done by irradiating the skin by Nd: YAG laser ( Carl Zeiss, Germany ) with a wavelength of 1064 nm, a repeated non pulsed continuous 20-s irradiation and a spot size of 8 mm. The aim of this technique is to raise the temperature of living skip, including the wart, from its normal level to about 45░C. This is easily accomplished by using the Nd: YAG laser beam which penetrates thermally to a depth of 4-7 mm (10). The surface temperature of the skin must be measured during the procedure, using a contact thermocouple and thermometer ( Fluke 51 Thermometer, John Fluke, USA ). It should not exceed 40-42 ░C [the subsurface temperature of the skin will reach about 45 ░C when the surface temperature is raised to 40 ░C (16)]. The required temperature was reached and maintained for one minute .
Modified Regensburg's Technique (MRT) .
On revising the medical records of patients receiving modifications of Regensburg's technique in our department. we found the following:
1. The best results were reached if Nd: YAG laser power is increased to 13W, 14W, and 15W. It was observed that when increasing the power, the temperature rise is more rapid and the required temperature is reached over a shorter time. However, no advantage of 14W and 15W over that of 13W was observed .
2. Decreasing the distance beyond 8 cm from the skin surface resulted in focusing of the laser beam which will lead to rapid healing resulting in laser vaporization with its risk of scarring. Increasing the distance more than 8cm, resulted in a wider spot size with less hyperthermic effect.
3. Prolongation of time of laser hyperthermia 2 min or more gave a lesser number of treatment sessions and a higher success rate. However, increasing the time more than 2min was intolerable by most of the patients if local anesthesia was not injected. 42 FIG .1B. Total cure after the first session using MRT Based on these data, the modification of RT (MRI) used in this study consisted of irradiating the lesion with an Nd: YAG laser beam with a power of 13 W, a spot size of 8mm, and a surface temperature of 40 ░C which is reached and maintained for 2 min.
Patients
ĀĀĀForty patients with warts (Table I) were enrolled in this study, 13 of them had verrucae vulgaris involving forearm and hands with a total of 100 lesions (mean+ SD of 7 615+3.042 lesions), 27 patients had multiple plantar warts with a total of 98 lesions (mean+SD of 3.917+- 792 lesions) . Patients with common warts were subdivided into two treatment subgroups, subgroup including 13 patients with 50 of the lesions treated by RT, and subgroup 1b including the same patients with the other 50 lesions treated by MRT. Patients with plantar warts were subdivided into subgroup 2a including 27 patients with 49 lesions treated with RT and subgroup 2b in which the remaining 49 lesions present in the same patients were treated with MRT.
ĀĀĀThe age of the patients ranged between 7 years and 52 years with a mean+SD of 25.650+12.052 years. Males constituted 47.5% of the test group (19 patients), while 52.5% were females (21 patients). In the common wart group, patient's age ranged between 7 years and 41 years with a mean+SD of 25 23+11.129 years. Sex distribution in this group showed that 46.2% were males (6 patients), and 7 patients were females (53.8%). In the plantar wart group, patient's age ranged between 7 years and 52 years with a mean+SD of 26.583+13.204 years. Sex distribution of this group showed that males were 48.2% and females were 51 8%. Results The cure rate was 100% in all 40 patients treated by MRT after two sessions while it was 95% after four treatment sessions using RT (Fig 1A, 1B, 2A, 2B, 3A, 3B) .The cure rate after one session was 60% in MRT and 15% RT subgroups and it was 100% after two sessions in MRT and 45% in RT. Fiftyfive percent of RT patients required a third session and 20% required a fourth session. Five percent of RT patients (two plantar wart patients) failed to be cured even after the fourth session (Histogram) (Fig4). No scarring, pigmentary changes, infection or other local complications were encountered in both techniques. However, two patients (5%) did not tolerate the MRT which necessitated giving them local anesthesia in the form of lidocaine I % F16 .2B. BOII1 left and right sided lesions were cured after two sessions with RT and MRT respectively FIG .3B. After the first session of MRT, most of the lesions were completely cured. The few remaining lesions completely disappeared after the second session. Discussion Wart treatment is often considered difficult because no specific antipapillomatous agents are available for therapy. The variety of treatment modalities available including keratolytics and antimitotic substances, immunotherapy, cryosurgery,C02 laser vaporization, complete surgical excision and even hypnotherapy, proves that so far there is no really satisfactory procedure for handling this common viral disease (17,21), Cryotherapy is a popular modality in North Europe, while C02 laser vaporization is becoming more popular in the US as a modality of wart treatment, but scarring, delayed healing time, the possibility of infection (HPV and HIV) and bleeding, are some of their known side effects(l8).
ĀĀĀĀHyperthermia is defined as an artificially induced increase in tissue temperature beyond the normal range. The use of hyperthermia in the treatment of malignant tumors was suggested by the observation that malignant tumor cells are more sensitive to heat than normal cells (22,23). Local hyperthermia requires the raising of the temperature to above 420C. When the temperature grossly exceeds 45OC, protein coagulation leads to thermal damage to the tissue. It was observed that temperatures above 42░C will increase the blood flow in the normal tissue but will decrease the tumor blood flow, thus causing inefficient dissipation of heat from the tumor, vascular occlusion and tumor necrosis(93,25).The decreased blood flow after hyperthermia will also result in a decrease in pH. This decrease in pH will enhance cell death and will inhibit the repair of thermally damaged cells(26).
ĀĀĀHyperthermia was used in the treatment of cutaneous leishmaniasis(8,9) and Mycobacterium chelonae infections Stern and Levine succeeded in causing regression of warts in a high percentage of cases using radiofrequency hyperthermia(11). They suggested that the exact mode of action of' heat therapy in warts still remains unclear. Either the virus is destroyed by the heat, by damage to the nutritive blood vessels or by the subsequent inflammatory response(11). Nd: YAG laser hyperthermia referred to as "laserthermia" (15, l6,27) is a new effective method for treating warts. In comparison to the CO2 laser, this method has considerable advantages. The skin remains intact, thus no bleeding takes place, no possibility of wound infection, and the treatment is not followed by scarring . Also there is no possibility of infection (HPV or HIV) from the fume as seen with CO2 laser vaporization. Pfau et al. tried their technique (Regensburg's technique ) in 31 patients suffering from recalcitrant common warts with a success rate of 77.4% with restriction of treatment sessions to only three sessions(l5). On comparing the results of our study on using RT with that of Pfau et al. we found that the cure rate was 95% compared to 77.4 % . This difference may be attributed to two factors, the first factor was the criteria of patient selection in which they selected only patients with recalcitrant warts while in our study patients were randomly chosen. The second factor is the number of treatment sessions which was restricted to three sessions in their work while we continued to a fourth session when needed. In our study on comparing RT & MRT after the second session, cure rate was found to be 45% and 100% respectively. Those who were not cured by 2 sessions of RT needed a third session in 55% and a fourth session in 20%. Five percent. of RT patients failed to be cured even after the fourth session. The big difference in cure rates after the second session between RT and MRT (45% and 100%) could be explained by the difference in the technique. In the former, the power energy used was 10W and the reached temperature (40░C) was maintained only for one minute while in the latter, the power was 13W and the reached temperature was maintained double the time i.e. for two minutes. Thus magnifying the noxious effects of laserthermia on the virus and/or the target tissue. Despite the near figures of cure rates between RT and MRT (95% and 100%) yet the number of treatment sessions favors the MRT. Absence of side effects like scarring, pigmentary changes, secondary infection and other local complications goes in accord with other studies which utilized hyperthermia in treatment of wartsĀĀĀ Ā( l5,16). In our opinion the intolerance of two patients (5%) for MRT except after local anesthesia, does not affect its position as a highly successful short timed and safe modality in wart treatment.
Fig.1A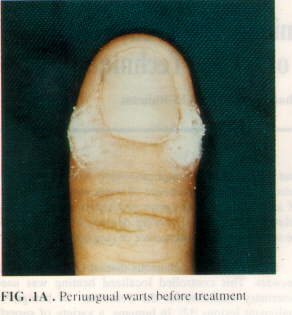 Fig.1B
Fig.1B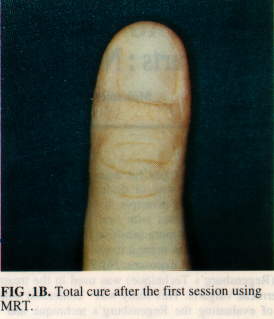 Fig.2A
Fig.2A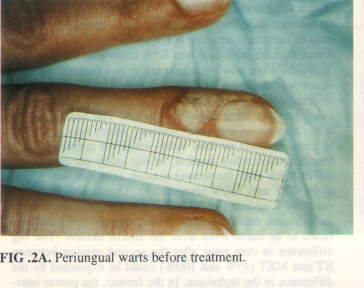 Fig.2B
Fig.2B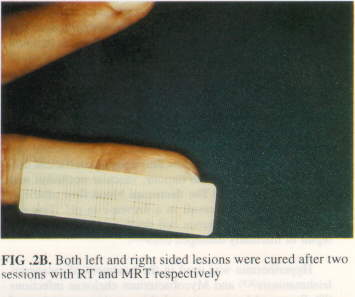
Fig.3A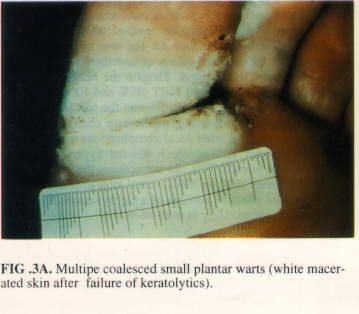 Fig.3B
Fig.3B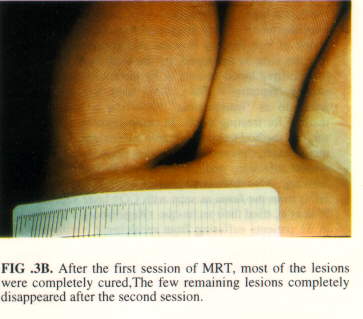 Table.1
Table.1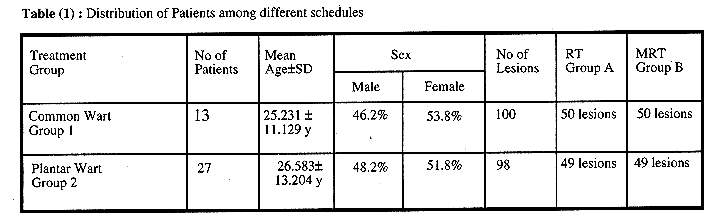 Fig.4
Fig.4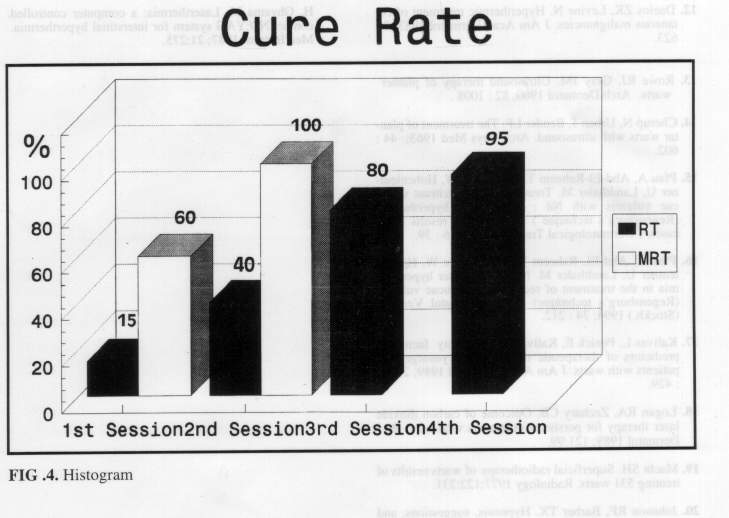
References
1. Highet and kurtz :Viral infections. In text book of dermatology Champion RH; Burton JL and Ebling FJG (eds) Black well scientific publications. London Edinburgh Boston Melbourne Paris Berlin Vienna 1992:867.
2. Bunney MH. Viral warts: their biology and treatment. Oxford University Press 1982; 134.
3. Leuker DC, Kainer, RA. Hyperthermia for the treatment of dermatomycosis in dogs and cats. Vet Med 1981; 16: 658
4. Grier RL, Brewer WG Jr,Thielen GH. Hypertherrnic treatment of superficial tumors in cats and dogs. JA Vet Assoc 1980: ]77: 2?7
5. Kainer RA. Current concept in the treatment of bovine occular squamous cell tumors. Vet Clin North Am 1984: 6 : 609.
6. Storm KF, Kaiser LR, Goodnight JE. Thermotherapy for melanoma metastases in liver. Cancer 1982 49: 1243 7. Lidholm CE, Kjellan E, Nilson P, Hertzman S. Microwave induced hyperthermia and radiotherapy in human superficial tumors - clinical results with a comparative study of combined versus radiotherapy alone. Int. J. Hyperthermia 1987:3:393
8. Neva FA, Petersen EA, Corsey R, Bogsert H, Martinez D. Observation of local heat treatment for cutaneous leishmaniasis . Am J Trop Med 1984: 33: 800.
9. Junaid AJN. Treatment of cutaneous leishmaniasis with infrared. Int J Dermatol 1986; 25: 470.
10. Levine N, Rothschild JG. Treatment of mycobacterium chelonae infection with controlled localized heating J Am Acad Dermatol I 991 ;24: 867.
11. Stern P, Levine N. Controlled localized heat therapy in cutaneous warts Arch Dermatol 1992: 12R 945.
12. Daelos ZK. Levine N. Hyperthermic treatment of cutaneous malignancies. J Am Acad Dermatol 1983; 9:
13. Rowe RJ. Gray JM. Ultrasound therapy of planter warts Arch Dermatol 1960: 82: 100X .
14. Cherup N, Urban J, Bender LF. The treatment of plantar warts with ultrasound. Arch Phys Med 1963; 44: 602.
15. Pfau A. Abd-EI-Raheem TA, Baumler W, Hohenleutner U, Landthaler M. Treatment of recalcitrant verrucae vulgaris with Nd: YAG laser hyperthermia (Regensburg's technique ) - preliminary results in 31 cases. J Derni3tological Treatment 199:;: 6: 39.
16. Pfau A, Abd-EL-Raheem TA. Baumler W, Hohenleutner U, Landthaler M. Nd: YAG laser hyperthermia in the treatment of recalcitrant verrucae vulgaris Regensburg's techni4ue) . Acta Dermatol Venerol. (Stockh.) 1994: 74: 212.
17. Kalivas L. Penick E, Kalivas J. Personality factors as predictors of' therapeutic response to cryosurgery in patients with warts. J Am Acad Dermatol 1989: 20 (3) :429.
18. Loyan RA, Zechaly CB. Outcome of carbon dioxide laser therapy for persistent cutaneous viral wart. Br J Dermatol 19X9: 121 99
19. Macht SH. Superficial radiotherapy of warts:results of treating 531 warts. Radiology 1977; 122:231.
20. Johnson RF, Barber TX. Hypnosis, suggestions, and warts:an experimental investigation implicating the importance of 'believed-in efficacy'.Am J Clin Hypn 1978:20:165.
21. Litt JA. Don't excise-excorise: treatment of subungual and periungual warts. Cutis 1978:22:673.
22. Giovenella BC. Stehlin JS, Morgan AC. Selective lethal effect of supranormal temperatures on human neoplastic cells. Cancer Res. 1976; 36:3944.
23. Emami B. Nussbaum GH, Tenhaken RK, Hughes WL. Physiologic effects of hyperthermia: response of capillary blood flow and structure to local tumor heating. Radiology 1980: 137:805.
24. Eddy HA. Alterations in tumor microvasculature during hyperthermia. Radiology 1980: 137:515.
25. Song CW. Kang MS,Rhee JG, Levitt SH. the effect of hyperthermia on vascular function, pH and cell survival. Radiology 1980: 137:795.
26. Song CW. Physiologic factors in hyperthermia. Monogr Natl. Cancer Inst. 1982: 61: 169.
27. Diakuzono N, Joffe SN, Taijri H, Suzuki S, Tsunekaw 46 H, Ohyama M. Laserthermia: a computer controlled contact ND:YAG system for interstitial hyperthermia. Med Instrum 1987; 21:275.
{kind=link}