CASE REPORT
SIDE LYING TRACTION AND MOBILISATION FOR ACUTE LUMBAR PAIN.
KEY WORDS
Traction, mobilisation, manual therapy, lumbar spine, acute low back pain.
INTRODUCTION
The purpose of this case study is to introduce readers to a new procedure for acute lumbar pain which was particularly effective in the treatment of this patient, a young clerical worker who had a sudden onset of severe radiating lumbar pain after twisting her back. It is a technique I have used successfully on regular occasions with similar patients.
While traction and side lying mobilisation are nothing new, the integration of these two techniques appears to have been an effective therapy for both reducing severe, acute pain and in quickly restoring mobility to this patient.
THE PATIENT
The patient was a fit 23 year old female clerical worker. Although in some distress with her back pain, she remained positive and motivated to return to work. She had a one day history of twisting her back while getting into her car. She had experienced sudden low back pain, with radiation of pain into the right buttock and posterior thigh extending to the right ankle, plus radiation into the left buttock and left upper posterior thigh. (Figure one). Her pain was severe and constant, with marked restriction of all movements. The pain was relieved slightly by standing and by lying. Pain was exacerbated by forward bending, rising to stand from a sitting position; and walking. At night the pain eased slightly but sleep was disturbed. Coughing or sneezing had not occurred so she was unable to say whether either would exacerbate the pain. There were no paraesthesiae or lower limb motor weakness. The acute pain prevented her from performing her normal occupation, a clerical job which was mainly sedentary. She had suffered a similar episode of low back pain three years previously which was successfully treated by physiotherapy in Australia. She had been prescribed Voltaren and Norflex tablets.
General health was excellent, she was not pregnant, on no other medication and bladder and bowel function were normal.
Observation:
The patient’s gait was affected by the acute back pain. In standing she had a slightly kyphotic lumbar spine. Sitting posture was too acute to assess. There was no observable sciatic scoliosis or lateral shift McLean IP, Gillan MG, Ross JC, Aspden RM, Porter RW (1996).
Active Movement Examination; standing:
Flexion - major loss of flexion and severe pain past 10% of normal range.
Extension - moderate loss of extension and mild pain past 30% of normal range.
Left Rotation - minimal loss of end range rotation, with no pain.
Right Rotation - minimal loss of end range rotation, with no pain.
Left Side Flexion - major loss of side flexion and severe pain past 20% of normal range.
Right Side Flexion - minimal loss of end range rotation, with no pain.
Repeated movements were not able to be assessed because of the severity of symptoms.
Diagnosis: On the basis of probability, a provisional diagnosis of acute posterior lumbar disc derangement was assumed. The pain pattern was consistent with the McKenzie category derangement five McKenzie (1981), the Quebec Task Force Classification number three, acute phase Spitzer (1986).
Goals of treatment: to reduce pain, restore mobility, restore normal function and facilitate return to normal employment. Verbal consent was obtained prior to all procedures.
INTERVENTION
Description of Side Lying Traction and Mobilisation Procedure:
This is a gentle procedure which should cause the patient no discomfort. The patient is asked to report any increase in pain or peripheralisation of symptoms, in which case the procedure is discontinued.
1. The patient is asked to lie with the knees together, painful side down and the hips flexed to about 45 degrees. The head is supported with a pillow to keep the spine in as straight a line as feasible. The pelvis and thorax are not rotated relative to each other.
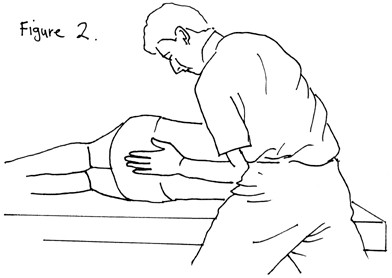
In this procedure the therapist is positioned behind the patient, facing the patient’s feet. Using a soft foam square for comfort and improved adhesion, the heel of the hand is placed on the lumbar spine centrally at the level of the intervertebral disc between the fourth and fifth lumbar vertebrae (L4/5). The supraspinous ligament is nestled between the therapist’s pisiform and trapezium. The therapist’s elbow is braced against the anterior superior iliac spine. For a left side-lying patient, the therapist is pushing with the right hand/right hip. For a right side-lying patient, the therapist is pushing with the left hand/left hip.
The therapist then adjusts the height of the couch or changes position so that the force of traction is coming from the hips, horizontally via the forearm, using his or her body weight. This is illustrated in figure two with foam removed for clarity of hand position. A series of eight firm but not forceful sustained tractions of four seconds duration are performed. There is not a great deal of movement. Ideally there should be a sensation of taking up the slack in the tissues, then releasing after four seconds. At all stages, the therapist checks for any increased discomfort or peripheralisation of symptoms.
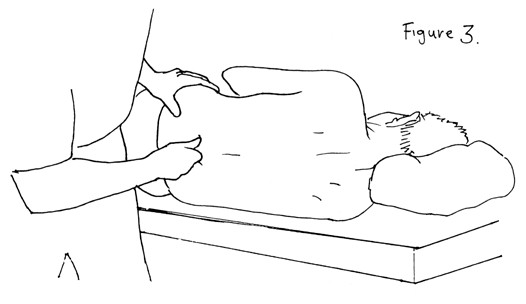
2. After traction, the patient’s pelvis is stabilised with the other hand, and extension mobilisations performed, again using a foam square for patient comfort. These mobilisations are in a postero-anterior plane, the force coming from the therapist’s free hand which is clenched into a fist and a V formed between the thumb and the flexed index finger as seen on figure 3 . The lumbar spinous process fits into the V and the force is transmitted to the articular pillars via the therapist’s horizontal forearm. If needed, the therapist can brace the elbow against the hip as described above, to increase stability and force. The extension mobilisations are performed at the level of L4/5 with the patient still in side lying. Five to six mobilisations will suffice. While it is wise to start with a gentle mobilisation, often there will be a surprising degree of pain free mobility of the segment and a stronger mobilisation causes no discomfort. Occasionally, these mobilisations are painful. If this happens, the traction is repeated and the pain should diminish.
After the extension mobilisation, a repeat set of eight tractions are given. The patient can then be re-assessed for range of motion and pain before being sent home with instructions regarding posture and maintaining the lumbar lordosis.
INTERVENTION
Day One, Treatment One: The patient was comfortable in right side lying (the most painful side down) with hips at 45 degrees flexion.
A hot pack was applied in this position for 15 minutes. After that, a series of eight side lying tractions were given and there was no pain during this procedure. Side lying extension mobilisation was attempted in this position but this was too painful. A repeat set of eight side lying tractions were given, again with no pain. The patient stated that she felt relief after side lying traction. At this point the patient was asked to lie prone in order to attempt the prone extension in lying exercise McKenzie (1981), but this was too painful. Another set of eight side lying tractions reduced the pain. The patient was sent home with posture instructions but strongly advised to avoid sitting. She was to use a lumbar roll if sitting was unavoidable.
Day Two, Treatment Two: The patient reported that she had experienced improved sleep, was walking without pain and had improved flexibility.
On examination, flexion range had improved to about 50% of normal, with moderate pain. Extension range was about 80% and mildly painful. All other movements were normal and pain free. Treatment was the same as for the previous day.
Day Five, Treatment Three: After a weekend with no treatment, the patient had felt a further decrease in pain. The pain had centralised Donelson R, Silva G, Murphy K (1990), Sufka et al. (1998) to the level of L4/5 with a radiating pain in the right posterior thigh present only when sitting for too long. There was no other radiation of pain.
Extension range had further increased to about 90%, flexion had improved to almost 80%. Treatment was as above plus prone active extension in lying, with seat belt fixation McKenzie (1981), plus side lying extension mobilisation .
Day Six, Treatment Four: There was a further decrease in the right leg pain.
Range of movement was much the same as the previous day. Treatment consisted of : a hot pack, side lying traction eight repetitions, side lying extension mobilisation, repeat set of side lying tractions, lumbar extension in lying with seat belt fixation McKenzie (1981).
Day Seven, Treatment Five: The patient reported she was pain free. On examination, her range of movement was full and pain free other than minimal stiffness on end range flexion only. (The patient said she had never been able to touch her toes and has always had a stiff back). Treatment as for treatment four.
The patient was discharged subject to a final assessment in two days time.
Day Nine: The patient rang to cancel the appointment as she was feeling fine and had returned to full time employment with all symptoms resolved.
IMPLICATIONS FOR PRACTICE
In this case, the patient was young, fit and healthy, all of which could lead to the assumption that the treatment worked rapidly because of natural history of the disorder.
I have observed, however, that a significant number of acute lumbar pain patients whom I have treated with this procedure have responded favourably regardless of age, state of health or fitness. I have frequently found that these patients were more comfortable lying on the painful side, in a degree of bilateral hip flexion, than in any other posture. Occasionally, the patient was more comfortable painful side up. In this case the treatment was commenced painful side up, then switched to painful side down once it was comfortable to do so.
The patients in which I have found this new treatment approach to produce the most beneficial response have been those who had acute unilateral or asymmetrical pain across the fourth and fifth lumbar intervertebral segment, with or without buttock and/or thigh pain, and/or pain extending below the knee.
I do not use this procedure for patients with central or symmetrical pain as the asymmetrical nature of the technique may cause peripheralisation of symptoms. Similarly, any patients with symptoms of frank nerve root impingement indicating disc prolapse are excluded.
Another group of patients which I have excluded from this treatment approach are those who exhibit a relevant sciatic scoliosis or lateral shift.
I suggest these patients are better dealt with using other lateral shift correction procedures Gillan MG, Ross JC, McLean IP, Porter RW (1998), Ross J (1998). While I have found that this technique can produce a rapid resolution of symptoms, I have seen it essentially as a ‘first aid’ treatment. Once the acute symptoms were settled, I have gone on to restore lumbar extension and maintain lordosis in accordance with the principles of the McKenzie (1981) system. In this way, the patient is still empowered with the responsibility for his or her back care maintenance.
While any explanation is hypothetical I suggest that, if one subscribes to the McKenzie model of intervertebral disc behaviour McKenzie (1981), Donelson R, Aprill C, Medcalf R, Grant W (1997) that this traction technique may reduce an internal displacement or an annular bulge of the intact intervertebral disc, by creating a negative pressure within the joint. Further, I suggest that the side lying mobilisation procedure subsequently aids restoration of the lumbar lordosis and that the combination of these two procedures creates an effect greater than the sum of its parts.
ACKNOWLEDGEMENTS
I would like to acknowledge encouragement given to me by Mark Laslett Dip. MT, Dip MDT., who has been a mentor for twenty years.
REFERENCES
Donelson R, Aprill C, Medcalf R, Grant W (1997) A Prospective Study of
Centralization of Lumbar and Referred Pain: A predictor of symptomatic
discs and anular competence. Spine 22:10
Donelson R, Silva G, Murphy K (1990) Centralisation Phenomenon: its
usefulness in evaluating and treating referred pain, Spine 15:3
Gillan MG, Ross JC, McLean IP, Porter RW (1998) The Natural History of
Trunk List, its Associated Disability and the Influence of McKenzie
Management. European Spine 7:6
McKenzie, R.A. (1981). The Lumbar Spine: Mechanical Diagnosis and
Therapy. Waikanae, New Zealand: Spinal Publications Ltd.
McLean IP, Gillan MG, Ross JC, Aspden RM, Porter RW (1996) A
Comparison of Methods For Measuring Trunk List. A simple plumbline is the
best. Spine 21: 14
Ross, J. (1998) Management of the lateral shift of the lumbar spine. Manual Therapy 3 2 62-66
Spitzer, W.O. (1986). Scientific approach to the assessment and management
of activity related spinal disorders. A monograph for clinicians. Report of the
Quebec Task Force on Spinal Disorders. Spine 12:7S
Sufka A. et al. (1998) Centralization of low back pain and perceived functional
outcome. Journal of Orthopaedic Sports Physical Therapy 27:3
Correspondence:
Philip L. Parker
PO Box 14328
Panmure
Auckland 1134
e-mail phil.parker@xtra.co.nz
Phone/Fax (09) 570 4976
{kind=link}
{kind=link}